The Bateman Horne Center (BHC) has been given the opportunity to read my blog posts in advance and to provide a comment.
Denna serie finns även på svenska. Du hittar den första delen via [denna länk].
Here is the BHC’s comment in full:
BHC’s Response to Mrs. Eremitage’s Blog Post
At the Bateman Horne Center (BHC), our mission is rooted in one guiding principle: to increase access to informed care for people with ME/CFS, Long COVID, and related conditions. That commitment is at the heart of our Clinical Care Guide: Managing ME/CFS, Long COVID, and IACCs-a 92-page resource designed to help clinicians deliver thoughtful, individualized care guided by decades of clinical expertise, scientific research, and patient insights.
A bullet point located in the orthostatic intolerance and dysautonomia chapter referencing neuroplasticity-based programs raised concerns for a member of the ME/CFS community, Mitt Eremitage. We appreciate the respectful dialogue with Mrs. Eremitage and the opportunity she has afforded us to clarify our intent:
- BHC does not recommend neuroplasticity programs as curative, primary, or as a standalone modality.
- We unequivocally reject any framing of ME/CFS or Long COVID as psychological disorders.
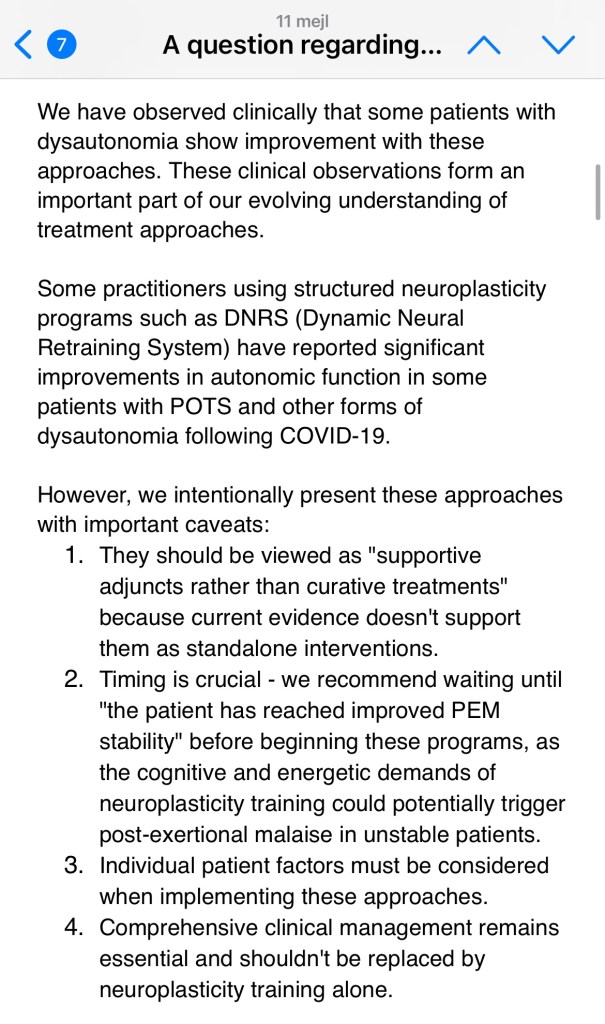
The reference in question is intended to apply to sympathetic overdrive as a part of the dysautonomia presentation. It notes that some patients—after achieving greater illness and post-exertional malaise (PEM) stability—may choose to explore nervous system regulation techniques as a supportive adjunct to care. We use the term PEM stability to mean that the patient is aware and knowledgeable of their exertional limitations and triggers, which lessens the frequency and severity of PEM.
As with any modality, modifications or adaptations may be required, ensuring the patient’s individualized needs and threshold for PEM are taken into consideration. This reflects the complex clinical reality we face daily and our responsibility to ensure patients are equipped with safeguards, not left to navigate these options alone.
We included this mention not to promote a particular method, but to responsibly frame the conversation for the patients and their providers who inquire about it.
The Clinical Care Guide provides patients and their providers with practical tools, interventions, and key considerations to support personalized management strategies.
BHC Clinical and Administrative Team
Unfortunately, the BHC’s comment is mostly a repetition of what they said in our previous dialog and they do not touch at all on the fact that the recommendation on brain training strongly contradicts their own guide. It is disappointing to see that an institution that otherwise so clearly stands up for both science and patient safety ends up this far off the mark when it comes to delineating itself against potentially harmful pseudoscientific methods.
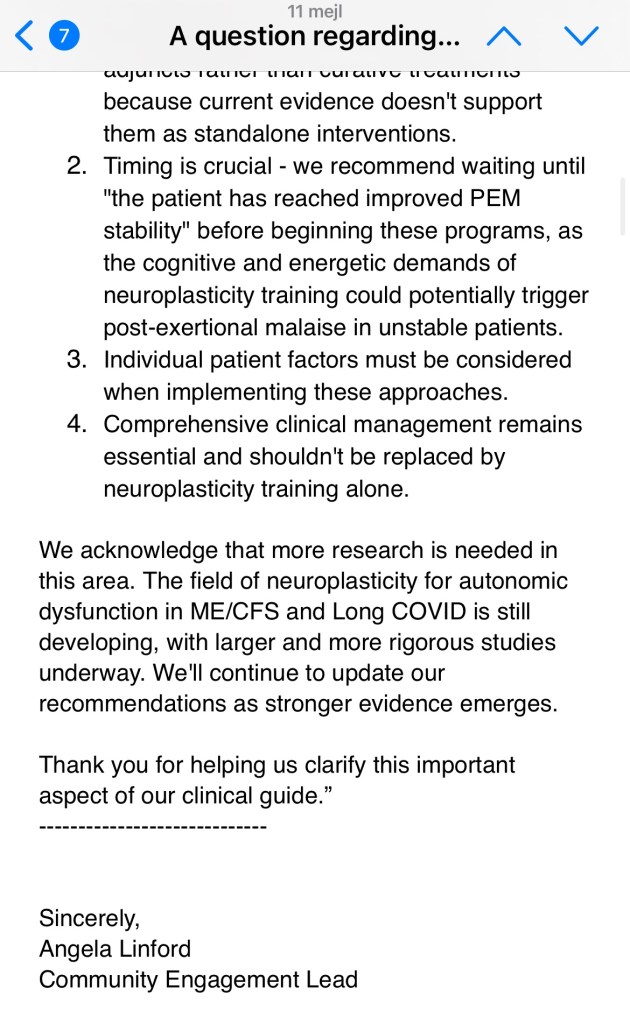
In the email to which the comment was attached, the BHC representative writes that in the next update of the guide they will add a statement that people participating in brain training programs may need to make adjustments to ensure that their individual thresholds are taken into account. In my opinion, this is not enough to compensate for the confusion that the discrepancy between the practical meaning of brain training programs and the advice on PEM in the BHC guide risks are creating.
On page 5 of the BHC Clinical Guide, providers are advised to adopt structured care approaches to ”navigate uncertainty effectively”. This refers to the clinical uncertainty surrounding diagnoses such as ME and long COVID. The fourth and final point on the list is about guiding patients in terms of resources to understand their illness.
They write:
“Guide patients toward reputable resources. Patients inevitably turn to online sources, where accurate information coexists with misinformation. Clinicians should recommend trusted organizations to empower informed decisionmaking.”
This seems rather bizarre because BHC themselves mix correct and incorrect information in their own guide. They give a vague recommendation on a unevidenced method that in many ways goes against their own sharp advice on PEM, without citing any sources.
This does not enhance patients’ ability to make informed choices but, on the contrary, contributes to confusion and increased risks of harm.
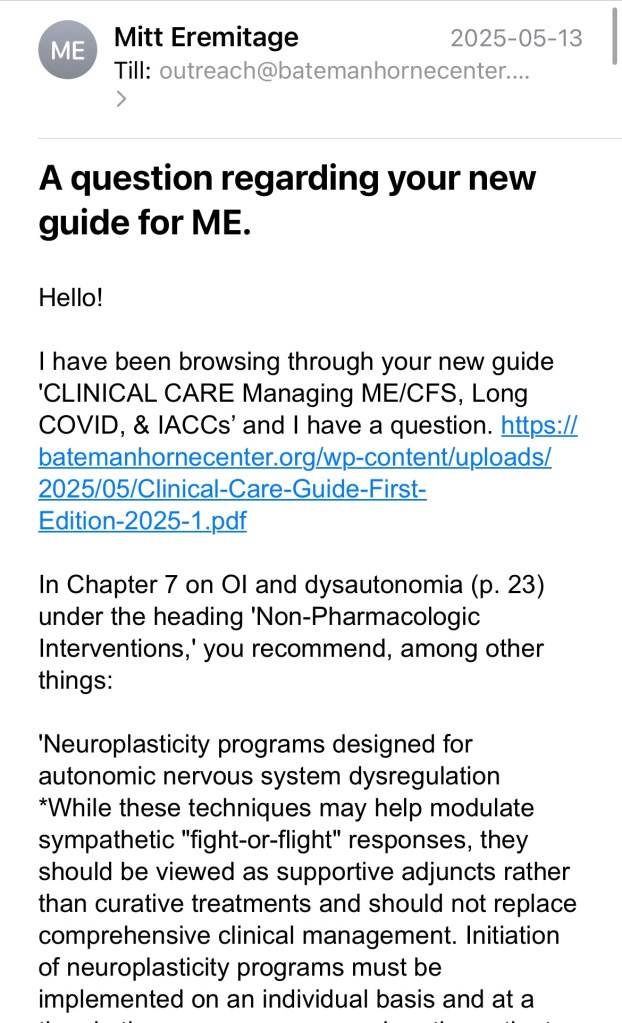
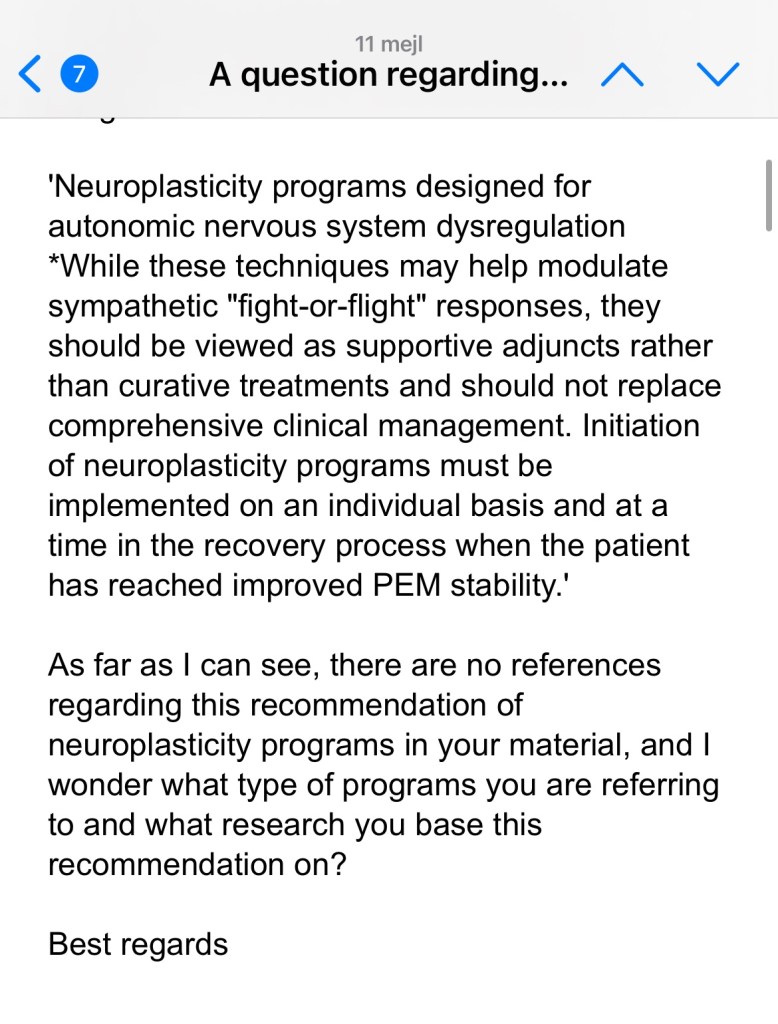
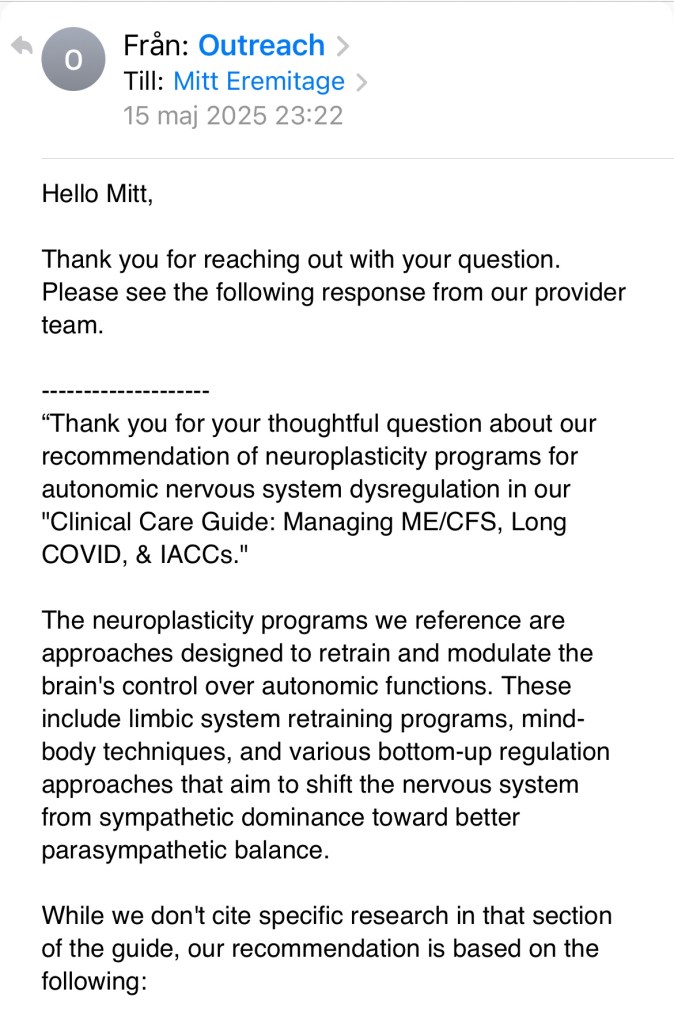
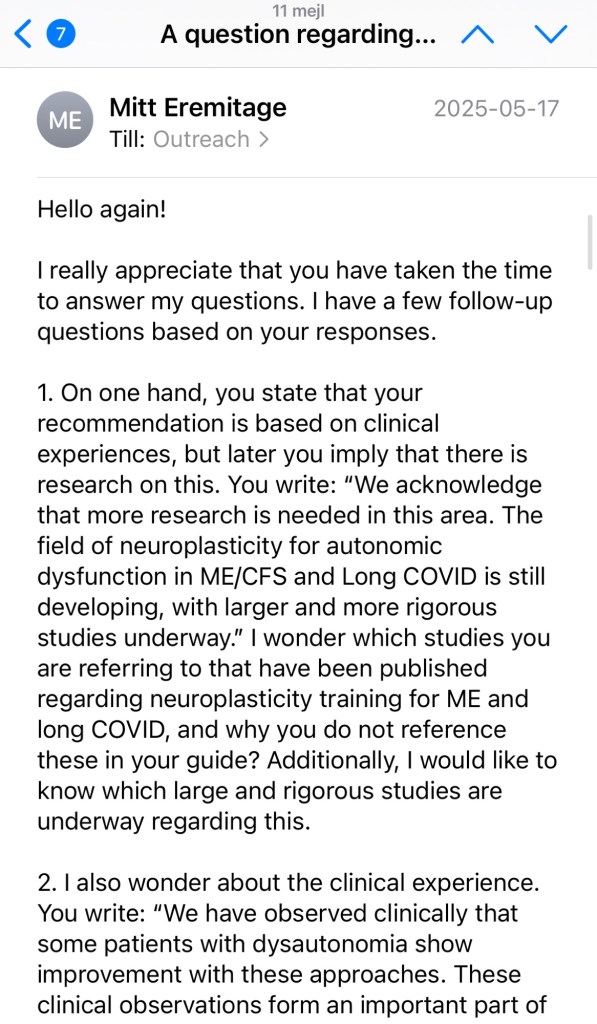
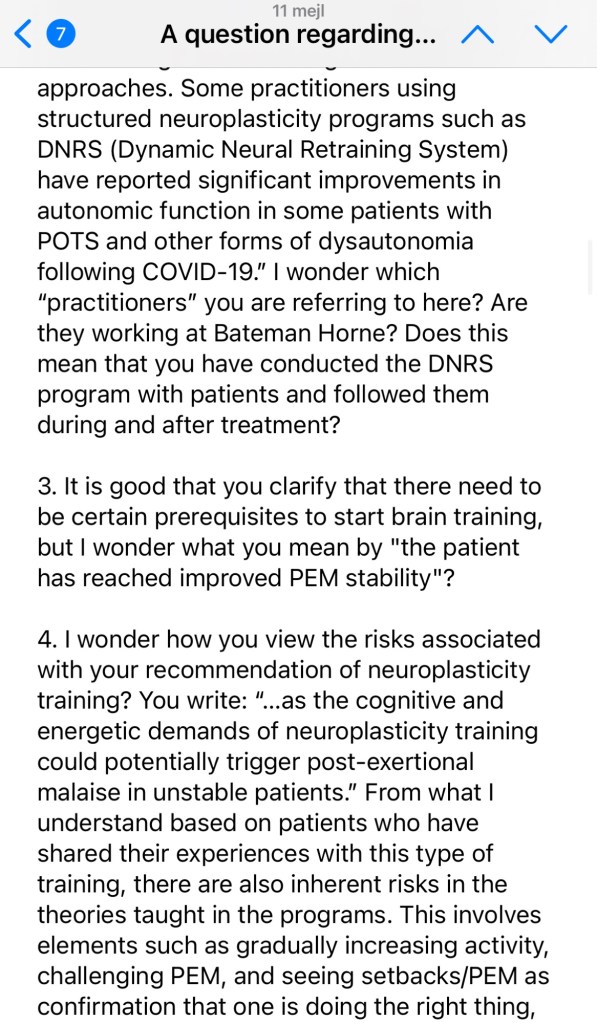
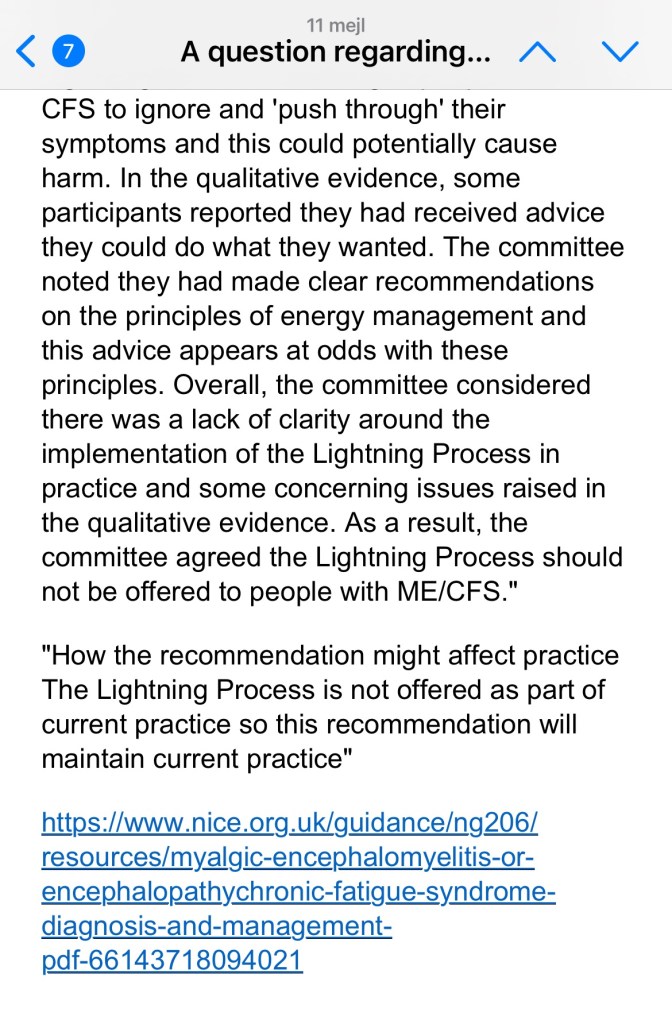
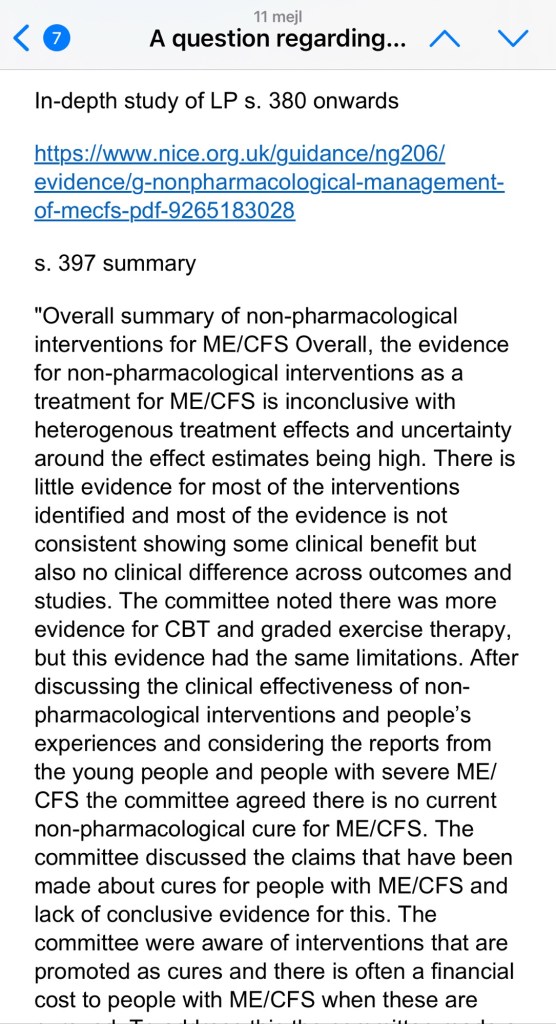
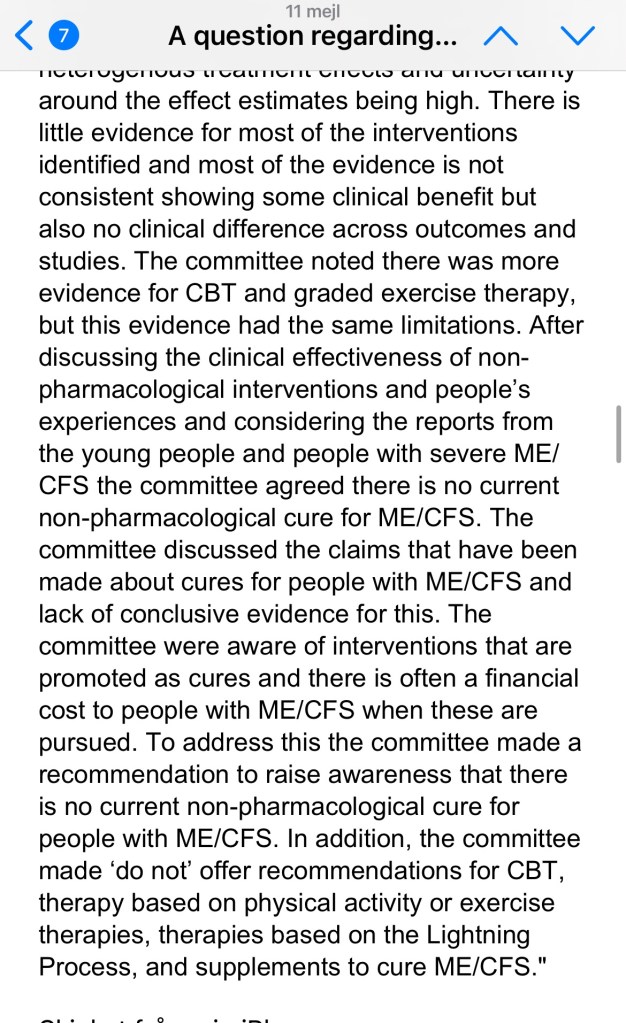
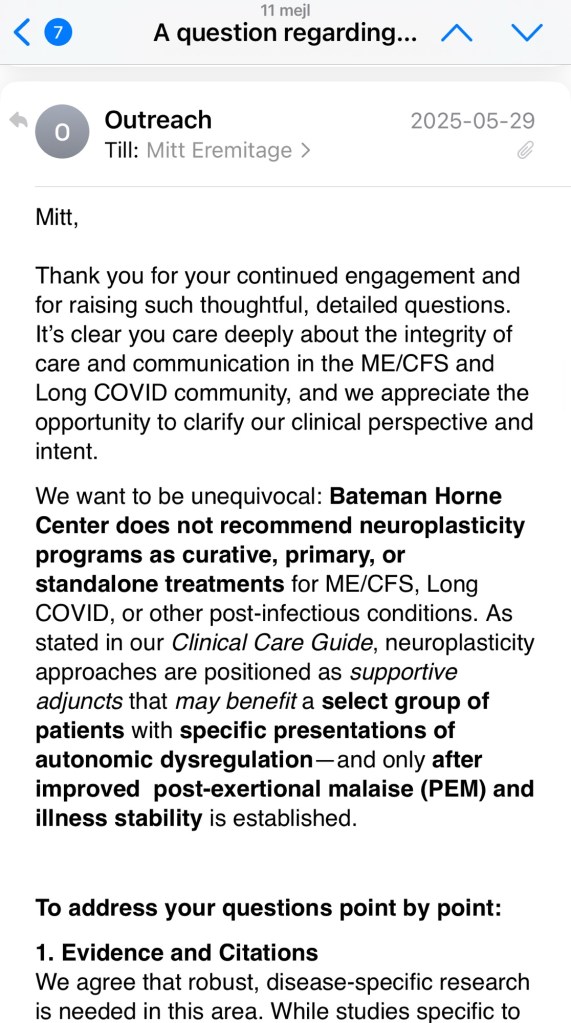
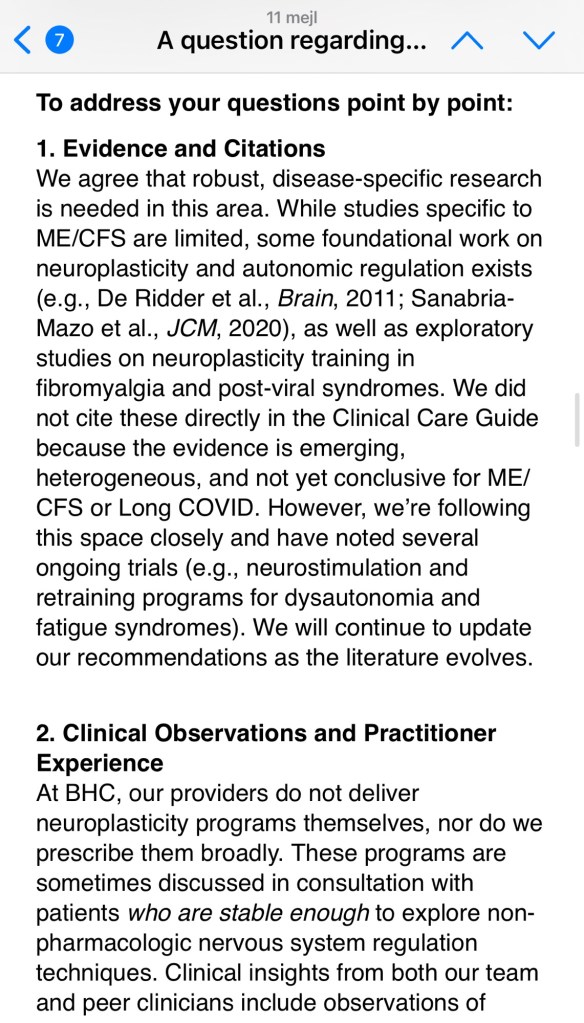
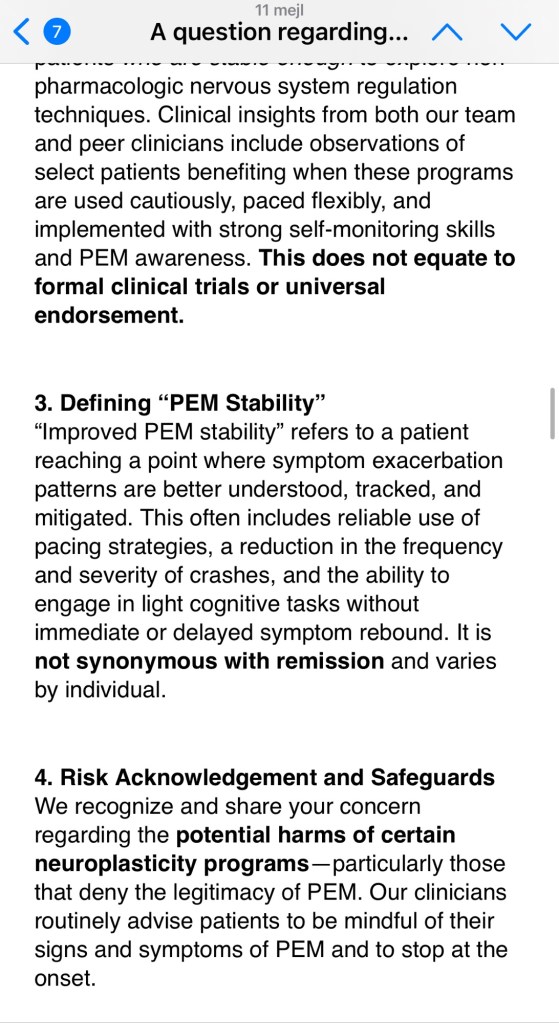
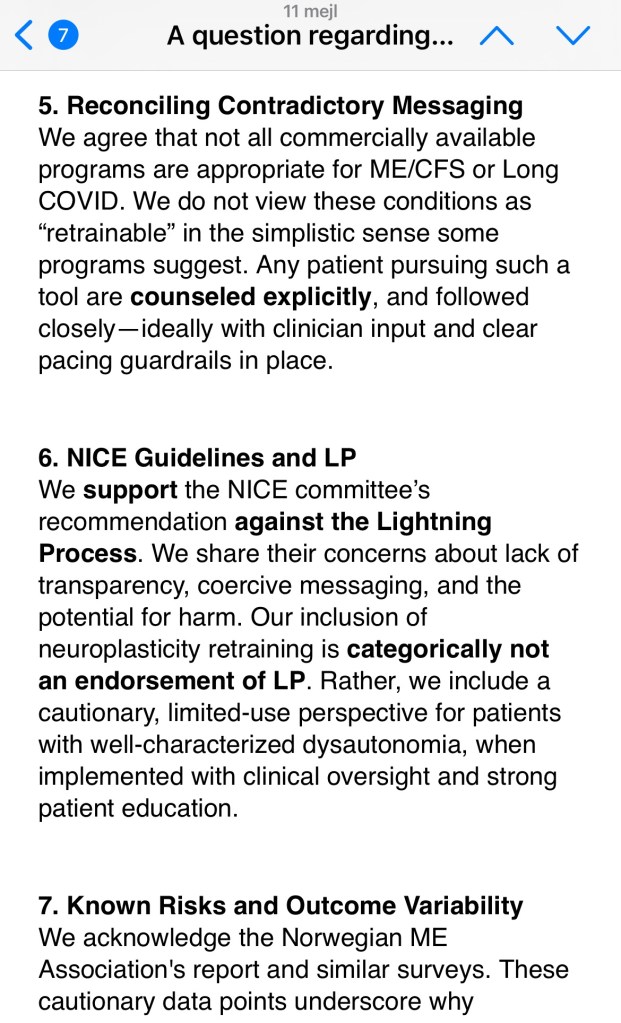
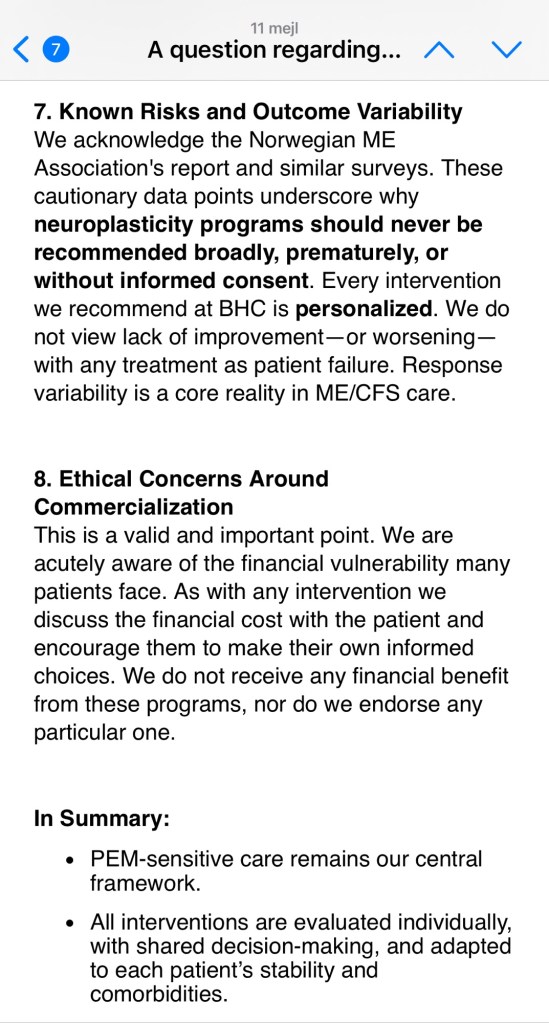
Screenshots of my dialog with the BHC in full:
Här hittar du alla inlägg samlade
Svenska:
- Rekommendation om hjärnträning i Bateman Horne Centers nya kliniska guide (del 1)
- Dialog med BHC angående rekommendationen om hjärnträning (del 2)
- En kritisk analys av BHC:s svar (del 3)
- Varför BHC:s rekommendation är riskfylld och motsägelsefull (del 4)
- BHC:s kommentar till mina inlägg om deras rekommendation av hjärnträning (del 5)
Engelska:
- Recommendation on brain training in Bateman Horne Centre’s new clinical guide (part 1)
- Dialogue with BHC regarding the recommendation on brain training (part 2)
- A critical analysis of BHC’s answers (part 3)
- Why the recommendation by BHC is risky and contradictory (part 4)
- BHC’s comment on my posts on their recommendation of brain training (part 5)
Upptäck mer från The ME Inquiry Report
Prenumerera för att få de senaste inläggen skickade till din e-post.
